Get Cna Shower Sheets Form
Key takeaways
When using the CNA Shower Sheets form, keep these key takeaways in mind:
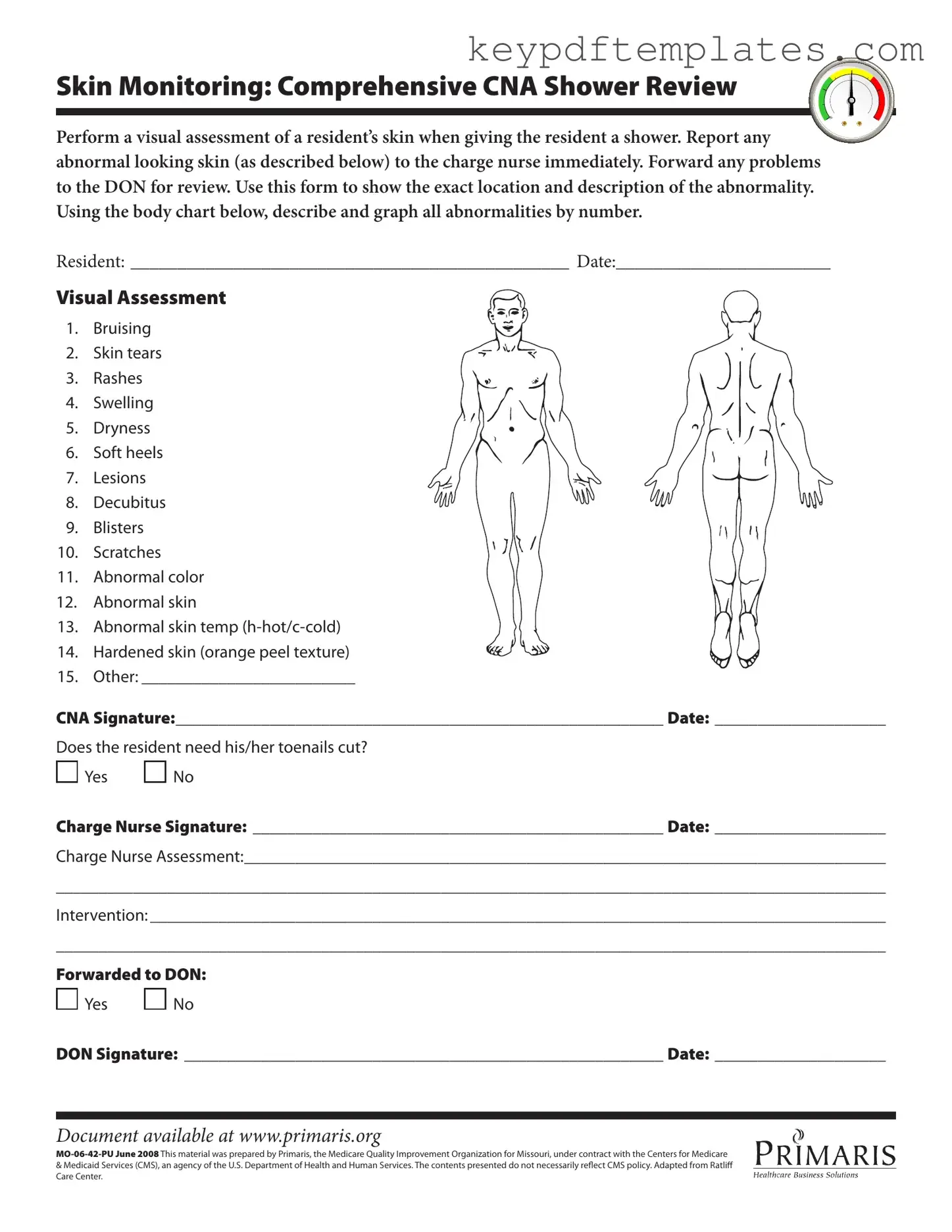
- Visual Assessment is Essential: Always perform a thorough visual assessment of the resident's skin during the shower. This helps in identifying any potential issues early.
- Document Abnormalities Clearly: Use the body chart provided to mark and describe any skin abnormalities. This ensures that all details are captured accurately for future reference.
- Timely Reporting is Crucial: If you notice any unusual skin conditions, report them to the charge nurse immediately. Quick action can prevent further complications.
- Follow-Up is Necessary: Make sure to forward any concerns to the Director of Nursing (DON) for further review and intervention as needed.
Similar forms
Skin Assessment Form: Similar to the CNA Shower Sheets, this document focuses on evaluating skin conditions. It records observations of skin abnormalities and provides a space for staff to note any issues that need further attention.
Incident Report: This form captures details of any incidents involving residents. Like the CNA Shower Sheets, it emphasizes the importance of documenting specific observations and actions taken regarding resident care.
Daily Care Log: Used by nursing staff, this log tracks daily activities and assessments of residents. It shares a similar purpose of monitoring resident well-being and documenting care provided.
Wound Assessment Form: This form specifically addresses wounds and injuries. It parallels the CNA Shower Sheets by requiring detailed descriptions and assessments of skin conditions that may require intervention.
Vital Signs Record: This document tracks residents' vital signs over time. It serves a similar function by documenting important health indicators and changes in resident conditions.
Care Plan Review: This document outlines the individualized care plans for residents. It is similar in that it requires ongoing assessment and documentation of resident needs and responses to care.
Medication Administration Record (MAR): This record details medications given to residents. Like the CNA Shower Sheets, it emphasizes the importance of accurate documentation in resident care.
- Operating Agreement: This essential document for LLCs outlines the management structure and procedures, ensuring compliance with state laws. For more information, visit Florida PDF Forms.
Behavioral Observation Form: This form is used to document any behavioral changes in residents. It shares the same focus on observation and reporting, ensuring that all aspects of resident care are monitored.
Misconceptions
Misconceptions about the CNA Shower Sheets form can lead to misunderstandings regarding its purpose and use. Here are eight common misconceptions, along with clarifications:
- It is only for documenting serious skin issues. Many believe that the form is only necessary when there are severe problems. In reality, it is important for documenting all types of skin conditions, even minor ones, to ensure comprehensive care.
- Only the CNA can fill out the form. Some think that only the Certified Nursing Assistant (CNA) is responsible for completing the form. However, collaboration with the charge nurse and the Director of Nursing (DON) is essential for accurate reporting and intervention.
- The form is optional. There is a misconception that using the form is optional. In fact, it is a required tool for monitoring residents’ skin health and should be utilized consistently during showers.
- Skin assessments are only necessary during showers. Some may believe that skin assessments should only occur during bathing. Skin monitoring should happen regularly, not just during showers, to ensure ongoing care.
- All skin abnormalities need immediate medical attention. There is a belief that every abnormality must be reported to a nurse immediately. While many do require prompt attention, some may not need urgent care but should still be documented.
- The form is not useful for tracking changes over time. Some individuals think that the form is only for immediate assessments. In truth, it serves as a valuable record for tracking changes in a resident's skin condition over time.
- Only visible issues need to be recorded. Many assume that only visible skin problems should be documented. However, changes in skin temperature or texture are also important and should be included in the assessment.
- Once filled out, the form does not need to be revisited. It is a common misconception that the form is a one-time assessment. In reality, it should be revisited and updated regularly to reflect the resident's current condition.
More PDF Templates
Triple Aaa International License - The permit provides you with driving privileges abroad.
When navigating the complexities of a divorce, it is crucial to understand the Florida Divorce Settlement Agreement form, as this document provides clarity on issues like asset division, child custody, and support obligations. For more information on how to properly complete this essential form, you can visit https://allfloridaforms.com/.
Complaint for Divorce Form Michigan - The form encapsulates crucial family law principles while remaining user-friendly.
Form Specs
| Fact Name | Description |
|---|---|
| Purpose | The CNA Shower Sheets form is used to document skin assessments during resident showers. |
| Skin Monitoring | It requires a visual assessment of the resident's skin, noting any abnormalities. |
| Immediate Reporting | Any abnormal findings must be reported to the charge nurse right away. |
| Documentation | The form includes a body chart for graphing the location of any abnormalities. |
| Signature Requirements | The CNA and charge nurse must sign and date the form after completing their assessments. |
| Forwarding Issues | Any problems found must be forwarded to the Director of Nursing (DON) for further review. |
| State Regulations | This form is governed by Missouri state laws regarding nursing and resident care. |
Documents used along the form
When working in a healthcare environment, particularly in facilities that provide care for residents, several important forms accompany the CNA Shower Sheets form. Each document plays a crucial role in ensuring the well-being of residents and maintaining accurate records. Below is a list of these documents, along with a brief description of each.
- Resident Care Plan: This document outlines the individualized care strategies for each resident. It includes specific goals, interventions, and the responsibilities of the care team to address the unique needs of the resident.
- Skin Assessment Form: Used to document the condition of a resident’s skin during routine checks, this form allows caregivers to record any changes over time, ensuring that skin integrity is monitored closely.
- Incident Report: This form is filled out when an unusual event occurs, such as a fall or injury. It helps in tracking incidents and implementing preventive measures to enhance resident safety.
- RV Bill of Sale: This form is essential for recording the sale of a recreational vehicle and provides legal evidence of ownership transfer. For anyone looking to buy or sell an RV, it’s crucial to complete this form, which you can find here: https://txtemplate.com/rv-bill-of-sale-pdf-template/.
- Daily Log: Caregivers use this form to record daily activities, observations, and any changes in a resident’s condition. It serves as a communication tool among staff members.
- Medication Administration Record (MAR): This document tracks all medications given to residents. It includes details such as dosage, time of administration, and any reactions noted, ensuring medication safety and compliance.
- Vital Signs Record: Caregivers use this form to log vital signs, such as blood pressure and heart rate. Regular monitoring helps in assessing the overall health status of residents.
- Fall Risk Assessment: This form evaluates a resident's risk of falling. It includes factors such as mobility, cognitive function, and previous fall history, aiding in the development of preventive strategies.
- Nutrition Assessment Form: This document is used to evaluate a resident's nutritional needs and dietary preferences. It helps in planning meals that meet individual health requirements.
These forms collectively contribute to a comprehensive approach to resident care, ensuring that each individual's needs are met effectively. Proper documentation is essential for maintaining high standards of care and facilitating communication among healthcare providers.